Dementia and Alzheimer’s disease are often used interchangeably in conversation, yet they represent distinct medical concepts that affect millions of families worldwide. While approximately 55 million people currently live with dementia globally, Alzheimer’s disease accounts for 60 to 70 percent of these cases, making it the most common cause but not the only form of cognitive decline.
Understanding the precise distinction between these terms shapes everything from diagnosis to treatment planning. Dementia describes a syndrome—a collection of symptoms affecting memory, thinking, and social abilities severely enough to interfere with daily functioning—whereas Alzheimer’s is a specific neurodegenerative disease characterized by distinct pathological changes in the brain.
This distinction matters because not all dementia stems from Alzheimer’s pathology, and some forms of cognitive impairment may even be reversible when caused by vitamin deficiencies, medication interactions, or thyroid problems rather than permanent neurodegeneration.
What Is the Difference Between Dementia and Alzheimer’s?
- Dementia functions as a syndrome rather than a single disease, encompassing multiple underlying conditions.
- Alzheimer’s disease represents the leading cause of dementia but constitutes only a portion of total cases.
- Vascular dementia, Lewy body dementia, and frontotemporal dementia account for significant percentages of non-Alzheimer’s cases.
- Accurate diagnosis requires biomarker testing for Alzheimer’s, while dementia is diagnosed clinically based on symptom patterns.
- Risk reduction strategies overlap between conditions, focusing on cardiovascular health and cognitive engagement.
- Mixed dementia—Alzheimer’s coexisting with other pathologies—complicates straightforward categorization.
| Fact Category | Dementia Overview | Alzheimer’s Specifics |
|---|---|---|
| Global Impact | 55 million affected worldwide | 60–70% of dementia cases |
| Primary Characteristic | Cognitive impairment interfering with daily life | Memory loss targeting hippocampus initially |
| Biological Markers | Varies by type | Amyloid-beta plaques, neurofibrillary tangles |
| Age Risk | Increases with age | Doubles every 5 years after age 65 |
| Genetic Factors | Varies by dementia type | APOE ε4 allele increases susceptibility |
| Diagnostic Method | Clinical cognitive testing | Biomarker confirmation (PET, CSF analysis) |
| Treatment Focus | Symptom management, underlying cause if reversible | Symptomatic relief, emerging disease-modifying drugs |
| Prognosis | Depends entirely on cause | Progressive decline over 4–8 years post-diagnosis |
Symptoms of Dementia vs Alzheimer’s
Early Signs and Memory Patterns
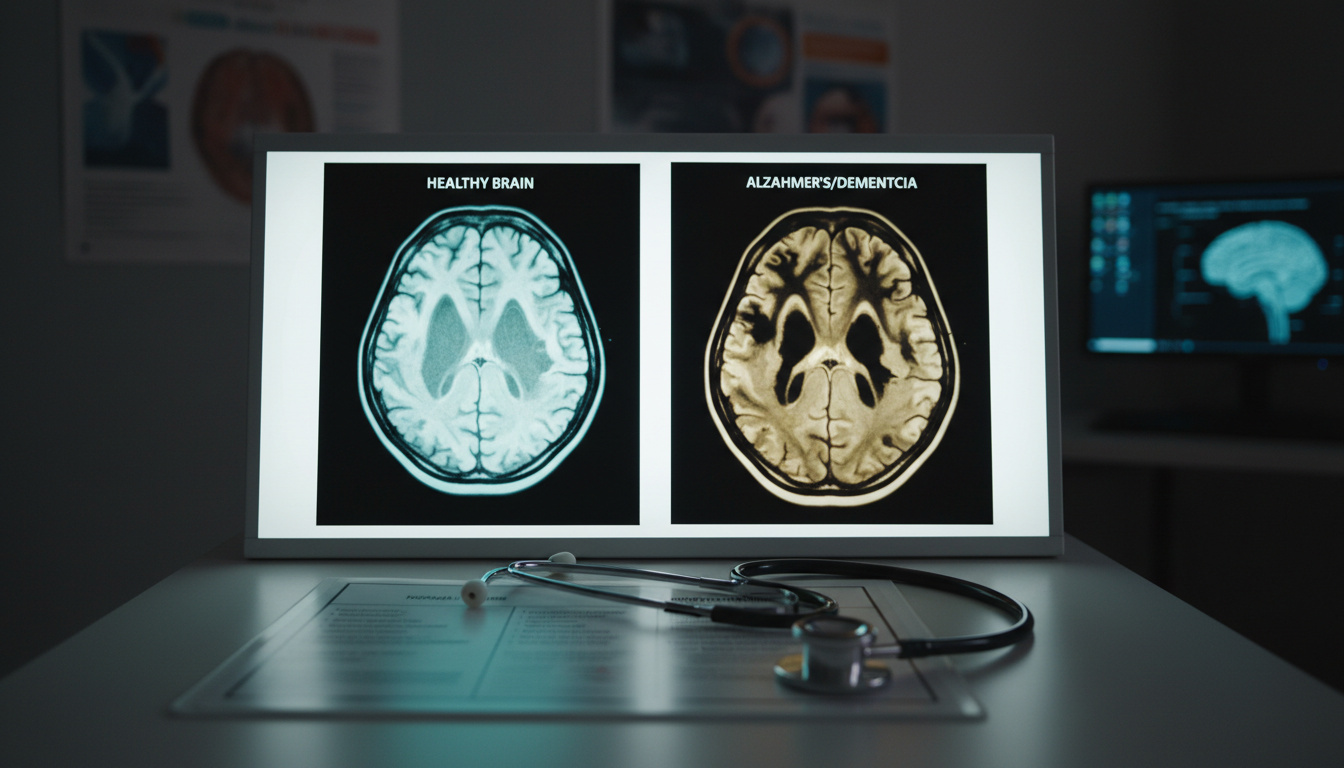
Alzheimer’s disease typically announces itself through specific memory impairments, particularly difficulty remembering recent events while older memories remain intact. This pattern reflects early damage to the hippocampus, the brain region responsible for forming new memories. According to the clinical literature, individuals may repeatedly ask the same questions or rely increasingly on memory aids for tasks they once managed independently.
Other forms of dementia present with different initial symptoms. Vascular dementia often follows a stepwise decline correlated with stroke events or cardiovascular incidents, while Lewy body dementia typically features visual hallucinations, fluctuating alertness, and movement difficulties early in the disease course. Frontotemporal dementia, by contrast, frequently manifests as personality changes or language difficulties rather than memory loss.
Behavioral and Cognitive Changes
As Alzheimer’s progresses into middle stages, language problems emerge, including paraphasias—substituting incorrect words or struggling to find familiar terms. Disorientation regarding time and place becomes common, alongside mood swings, loss of motivation, and behavioral issues. The National Center for Biotechnology Information notes that these symptoms reflect spreading neurodegeneration beyond the hippocampus into cortical regions governing language and executive function.
Late-stage Alzheimer’s brings severe memory loss, including failure to recognize close relatives, loss of long-term memory, and total dependence for basic activities of daily living. While other dementias can reach similar endpoints, the specific trajectory and predominant symptoms vary based on which brain regions sustain damage first.
Identifying Alzheimer’s-specific memory patterns allows for earlier intervention with cholinesterase inhibitors and participation in clinical trials for emerging therapies, potentially slowing progression during mild cognitive impairment stages.
Causes and Types: Dementia vs Alzheimer’s
Biological Mechanisms
Alzheimer’s disease develops through a cascade of protein misfolding events. Amyloid-beta plaques accumulate between neurons while tau proteins form neurofibrillary tangles inside cells, eventually triggering cell death and brain atrophy. Research published by the Alzheimer’s Association indicates these changes may begin 10 to 20 years before symptoms appear, during a preclinical phase detectable only through biomarker analysis.
Genetic factors play a significant role, particularly the APOE ε4 allele, which increases susceptibility though does not guarantee disease development. Environmental influences including diet, physical inactivity, and low cognitive engagement contribute to risk, interacting with genetic predispositions in complex ways. The National Institute on Aging emphasizes that advancing age remains the strongest risk factor, with the probability of Alzheimer’s doubling approximately every five years after age 65.
Other Dementia Types Beyond Alzheimer’s
Dementia encompasses several distinct pathologies beyond Alzheimer’s. Vascular dementia results from impaired blood flow to the brain, often following strokes or chronic small vessel disease. Lewy body dementia involves abnormal deposits of the protein alpha-synuclein, causing symptoms that overlap with both Alzheimer’s and Parkinson’s disease. Frontotemporal dementia attacks the frontal and temporal lobes, leading to personality changes and language difficulties rather than initial memory impairment.
Mixed dementia—where Alzheimer’s pathology coexists with vascular changes or Lewy bodies—complicates diagnosis and treatment. According to federal health resources, autopsy studies reveal that mixed pathologies are more common than previously recognized, particularly in the oldest old.
Progression, Diagnosis, and Treatment Differences
Staging and Timeline
The 2024 National Institute on Aging and Alzheimer’s Association (NIA-AA) criteria define Alzheimer’s as a biological continuum rather than discrete stages. Clinical staging ranges from Stage 0 (asymptomatic with genetic risk) through Stage 6 (severe dementia). Biological staging uses Core 1 biomarkers—amyloid PET imaging or CSF/plasma p-tau measurements—to identify Alzheimer’s neuropathologic change before symptoms emerge.
Traditional clinical descriptions still reference early, middle, and late stages. Early-stage patients maintain independence but experience measurable memory difficulties. Middle stages bring loss of independence, increased falls risk, and wandering behaviors. Late-stage disease involves total care dependence, with average survival ranging from four to eight years following diagnosis, though individual trajectories vary significantly.
The 2024 diagnostic criteria revision represents a paradigm shift toward biomarker-driven diagnosis, allowing identification of Alzheimer’s pathology during preclinical phases decades before cognitive symptoms manifest, fundamentally changing clinical trial recruitment and treatment timelines.
Diagnostic Criteria
Dementia diagnosis remains primarily clinical, based on comprehensive cognitive testing and functional assessments. However, distinguishing Alzheimer’s from other dementias increasingly relies on biomarker confirmation. Amyloid PET scans, cerebrospinal fluid analysis, and emerging blood tests detect amyloid and tau pathology with improving accuracy. The Mayo Clinic emphasizes that structural MRI and metabolic PET imaging help rule out strokes, tumors, or other conditions mimicking dementia.
Probable Alzheimer’s dementia requires documented cognitive impairment without significant comorbidities that could explain symptoms. Possible Alzheimer’s applies when patients show atypical features or have coexisting conditions like cerebrovascular disease. This distinction guides treatment decisions and prognosis discussions.
Current Therapies
No current treatments cure Alzheimer’s or most progressive dementias. Symptomatic management includes cholinesterase inhibitors and the NMDA antagonist memantine, which temporarily improve cognition or slow decline in some patients. Antipsychotic medications may address behavioral symptoms but carry increased mortality risks in elderly dementia patients.
Emerging therapies specifically target Alzheimer’s pathology. The monoclonal antibody lecanemab received accelerated approval for clearing amyloid plaques in early Alzheimer’s, though access remains limited and requires biomarker confirmation of amyloid positivity. According to the World Alzheimer Report 2024, disease-modifying treatments remain unavailable for most patients globally, with symptomatic and supportive care constituting the standard of care. For those seeking natural remedies, information on Hausmittel gegen Schlafstörungen may be helpful.
Supportive interventions—including Mediterranean diets, regular physical exercise, social engagement, and cardiovascular risk management—demonstrate measurable benefits in slowing cognitive decline across dementia types. Caregiver support programs prove equally essential, given that dementia care costs continue rising worldwide.
While emerging Alzheimer’s therapies show promise, the World Alzheimer Report 2024 confirms no widespread disease-modifying treatments currently exist. Patients should maintain realistic expectations regarding symptom management versus disease reversal, particularly given the progressive and irreversible nature of Alzheimer’s pathology.
How Alzheimer’s Disease Progresses Through Stages
- Preclinical Phase (10–20 years): Amyloid plaques and tau tangles accumulate silently. Brain changes detectable only via biomarker testing, with no cognitive symptoms apparent.
- Mild Cognitive Impairment (MCI): Early symptoms emerge, particularly recent memory loss exceeding normal aging. Individuals may lose objects, forget appointments, or struggle with complex tasks while maintaining independence.
- Mild Dementia: Diagnosis becomes possible as daily functioning declines. Difficulty managing finances, medication errors, and repeated questioning characterize this stage.
- Moderate Dementia: Language problems intensify with paraphasias and word-finding difficulty. Disorientation, wandering, sleep disturbances, and behavioral changes require increased supervision.
- Severe Dementia: Total dependence for personal care. Patients lose ability to recognize family, communicate effectively, or control movement. Average survival ranges from four to eight years following initial diagnosis.
Sources: NCBI, Alzheimer’s Association Facts and Figures
Established Facts vs. Remaining Uncertainties
| Established Medical Consensus | Areas of Ongoing Uncertainty |
|---|---|
| Alzheimer’s disease causes 60–70% of dementia cases globally. | Precise triggers for sporadic late-onset Alzheimer’s remain unidentified. |
| Amyloid-beta plaques and tau tangles define Alzheimer’s pathology. | Whether amyloid causes the disease or represents a byproduct of other processes. |
| Biomarker testing (PET, CSF, blood) can confirm Alzheimer’s pathology. | Why some individuals with high amyloid loads remain cognitively normal. |
| Certain dementias (B12 deficiency, hypothyroidism) are reversible with treatment. | Exact mechanisms determining individual progression rates and cognitive reserve. |
| Risk doubles every five years after age 65 for Alzheimer’s. | Effective prevention strategies for those without genetic risk factors. |
| Lecanemab and similar drugs reduce amyloid in early Alzheimer’s. | Long-term clinical benefits and safety of disease-modifying therapies. |
Why the Distinction Matters for Healthcare Planning
The clinical distinction between dementia as a syndrome and Alzheimer’s as a specific disease fundamentally shapes medical care, legal planning, and family expectations. Accurate diagnosis determines whether patients might benefit from Alzheimer’s-specific therapies like lecanemab, which requires confirmed amyloid positivity, or whether addressing vascular risk factors could stabilize or improve cognition in mixed dementia cases.
Insurance coverage, clinical trial eligibility, and caregiver education all depend on precise terminology. The Centers for Disease Control and Prevention notes that distinguishing reversible causes of dementia—such as medication interactions, depression, or metabolic disorders—from progressive neurodegenerative diseases can prevent unnecessary suffering and healthcare costs. For specific medication safety concerns, review Why Is Linzess Dangerous – FDA Warnings and Key Risks.
Globally, the World Health Organization projects 139 million dementia cases by 2050, making accurate differential diagnosis increasingly critical for healthcare resource allocation. Understanding that Alzheimer’s represents the majority but not entirety of dementia cases helps families navigate the complex landscape of care options, from memory care facilities to home-based support systems tailored to specific dementia subtypes.
Expert Perspectives on Cognitive Decline
“Alzheimer’s disease is the most common cause of dementia, accounting for an estimated 60% to 70% of cases. While dementia describes a group of symptoms affecting memory, thinking, and social abilities, Alzheimer’s is a specific brain disease marked by the buildup of amyloid plaques and tau tangles.”
— National Institute on Aging
“The 2024 revision of the NIA-AA criteria represents a fundamental shift toward defining Alzheimer’s disease by its underlying biology rather than just clinical symptoms, enabling earlier detection and intervention.”
— Alzheimer’s Association Research Framework
Research from the National Academies of Sciences emphasizes that while risk reduction strategies show promise, no interventions currently cure or definitively prevent Alzheimer’s disease, highlighting the importance of accurate diagnosis for appropriate symptom management and family planning.
Understanding the Core Distinction
Dementia serves as the umbrella term describing cognitive decline severe enough to impair daily functioning, while Alzheimer’s disease represents the specific neurodegenerative pathology causing most—but not all—dementia cases. This distinction carries practical implications for treatment, with some dementia causes remaining reversible and others, like Alzheimer’s, requiring specific biomarker confirmation for emerging therapies. For related health concerns involving unexplained physical changes, see White Spots on Skin – Causes, Treatments and When to Worry.
Frequently Asked Questions
Can dementia be cured?
Some dementia types caused by vitamin deficiencies, thyroid disorders, or medication interactions are reversible with treatment. However, Alzheimer’s disease and most other neurodegenerative dementias currently have no cure, though treatments can manage symptoms.
How long do people live with Alzheimer’s?
Following diagnosis, individuals with Alzheimer’s disease typically survive four to eight years on average, though some live 20 years or more. Life expectancy varies based on age at diagnosis, overall health, and quality of care.
Is Alzheimer’s hereditary?
Genetics play a role, particularly the APOE ε4 allele which increases risk. However, having a first-degree relative with Alzheimer’s does not guarantee development of the disease, and most cases involve complex interactions between genetic and environmental factors.
Can you have dementia without Alzheimer’s?
Yes. Vascular dementia, Lewy body dementia, and frontotemporal dementia represent significant portions of non-Alzheimer’s cases. Additionally, some dementias stem from reversible causes like B12 deficiency or normal pressure hydrocephalus.
What foods help prevent dementia?
Mediterranean and MIND diets—emphasizing leafy greens, berries, nuts, whole grains, fish, and olive oil—correlate with reduced dementia risk. These patterns support cardiovascular health and may reduce amyloid accumulation in the brain.
How is Alzheimer’s diagnosed differently from other dementias?
Alzheimer’s diagnosis increasingly relies on biomarker detection through PET scans or cerebrospinal fluid analysis to identify amyloid plaques and tau tangles. Other dementias are diagnosed primarily through clinical symptom patterns and ruling out other conditions.
What’s the difference between senility and dementia?
Senility reflects outdated terminology implying that severe memory loss is a normal part of aging. Dementia describes pathological cognitive decline that exceeds normal aging and interferes with daily functioning, regardless of the underlying cause.
Are there new treatments for Alzheimer’s?
The monoclonal antibody lecanemab received approval for early Alzheimer’s, showing ability to reduce amyloid plaques. However, access remains limited, requires biomarker confirmation, and long-term clinical benefits remain under investigation according to 2024 reports.